Simulating Reusable Medical Equipment in Hospitals
Alice Ng
Supervisor: Dr. Michael O’Sullivan
Introduction
When surgical procedures are scheduled in hospitals, there is no rigorous allocation of equipment required to the future procedure. Due to this lack of planning, there may be times where the supply of equipment is not sufficient to meet demands. This can lead delays or cancellations of surgeries. My project was to investigate how Reusable Medical Equipment (RME) can be better managed at hospitals. This involved creating a Discrete Event Simulation to model the processes that are currently in place. The simulation can then be used to evaluate potential improvements to the system.
Types of Surgeries
At most hospitals, there are two main types of surgeries that are performed in operating theatres: elective surgeries and acute surgeries. Electives are surgeries that are planned for, and scheduled typically weeks in advance, for patients in a non-critical condition. Acute surgeries, on the other hand, are performed when patients arrive at hospitals unexpectedly, and need immediate medical attention.
Reusable Medical Equipment
There are various types of medical supplies that are used in the operating theatre. Reusable Medical Equipment (RME) are instruments that are owned by the hospital, and can be reused after surgeries. Between uses, they are processed in the hospital’s Central Sterile Supply Department (CSSD), where they are washed, re-packed and sterilised. These typically are kept together and are used as sets, and so I have also referred to these as instrument sets.
The CSSD has a finite number of machines, and so during peak hours, equipment having to queue. Generally queues are processed on a first in first out basis, but if there is an item that is needed urgently, it can be moved to the front any queues. This is a process called fast-tracking. But fast-tracking disrupts the workflow in the CSSD, causes delays for other equipment, and also puts staff under pressure to get the equipment ready in time for the surgery. Therefore it is desired to keep fast-tracking to a minimum.
Historical Surgical Schedule
A historical surgical schedule, provided by Middlemore Hospital, was used as the underlying input to drive the use of RME in the simulation model.
Equipment Lists
Simplified equipment lists were created for each procedure, to represent the expected resource demands.*
Python Processing
Python scripts were used combine the information from the historical surgical schedule and equipment lists to generate appropriate inputs to the JaamSim model.
* The actual equipment lists for each procedure could not be sourced within the time frame of this project. Thus, assumptions had to be made about how equipment is used. Due to these assumptions, this project will not generate results that accurately reflect the usage of RME. Instead, the results will demonstrate a proof of concept.
Equipment lists for a procedure arrive the day before the surgery, and the required equipment is claimed if available.
The entities with all of their equipment, move on to the operating theatres when it is their scheduled start time.
After the surgery is complete, the equipment are processed in a series of stations in the CSSD, where they are washed, packed, and then sterilised. These stations have service times modelled with uniform and triangular distributions.
Entities without all of their equipment will generate a request for the equipment to be fast-tracked. The fast-tracking process is modelled by having two queues, for each of the 3 CSSD stations, where any equipment in the fast-track queue is always processed first.
Once a fast-tracked item is returned to storage, it is claimed by the first procedure on the waitlist.
If there are still outstanding requests for equipment by the time the surgery is scheduled to start, it is assumed that the surgery is cancelled.
Results
Base Case
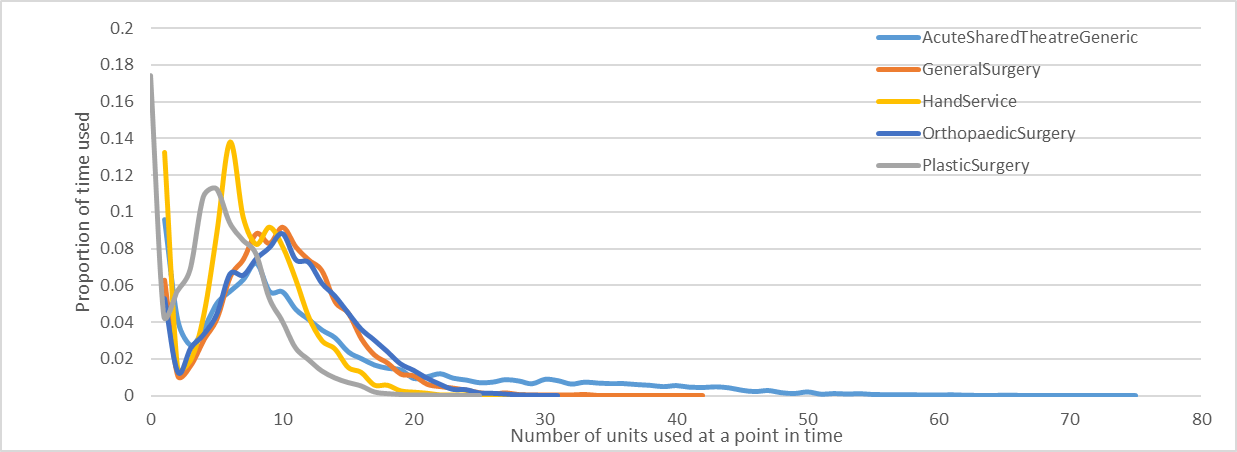
The simulation was run with an infinite capacity for all instrument sets. From this we could determine the maximum number of instrument sets needed to be held by the hospital, to avoid any fast-tracking. The resource utilisation for the 5 most frequently used instrument sets is shown below. It can be noted that the maxima are typically higher than the average utilisation. Demand distributions illustrate that there is a significant proportion of time in which there are none of an instrument set in use. The occasions in which resource requirements are greater are not as common – this is seen as the trailing tails on the right. Thus, having the maximum number of instrument sets available will result in low utilisation, with a lot of idle resource. This will come at a high cost to hospitals: there is an implicit cost from purchasing equipment, a holding cost from the storage space occupied, and an opportunity cost from money that could have been spent elsewhere.
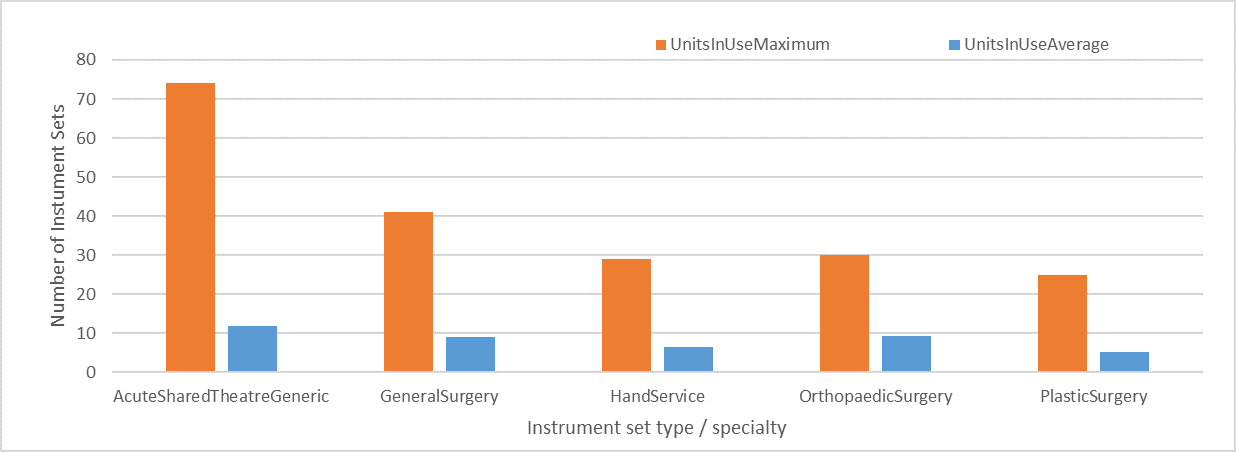
The maximum number vs average number of units of instrument sets used
The proportion of time a number of instrument sets has been used at once
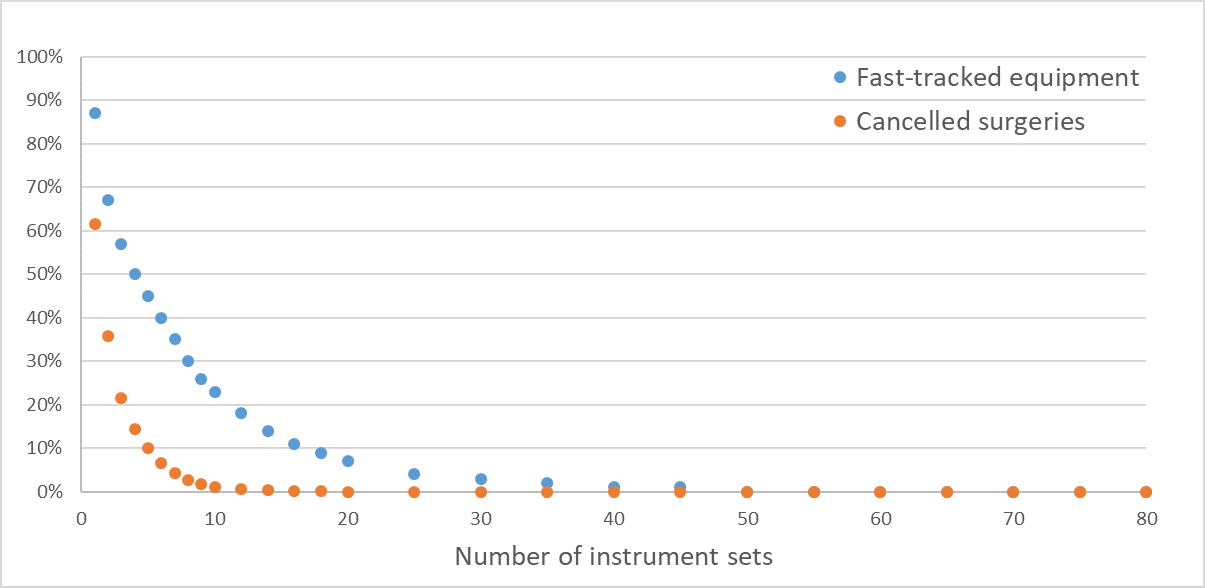
The simulation was then run with an increasing number of instrument sets available, to determine the effect of inventory levels on the following service levels:
- The percentage of total equipment processed in the CSSD, that needs to be fast-tracked
- The percentage of total surgeries that are cancelled, due to equipment not being ready in time
We see that as the number of instrument sets available increases, there is a decrease in the percentage of fast-tracks and surgery cancellations. It can be noted that eliminating fast-tracks completely is much more resource intensive than eliminating surgery cancellations.
CSSD Utilisation
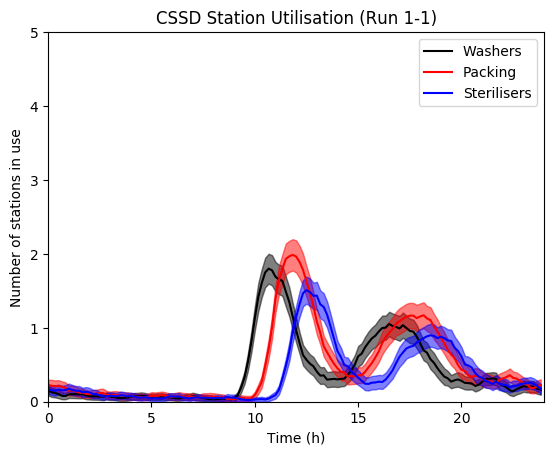
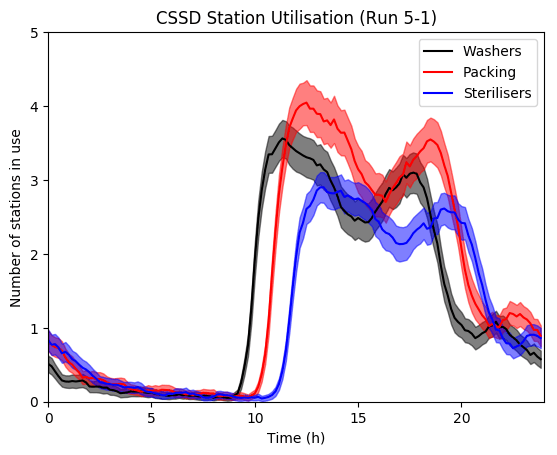
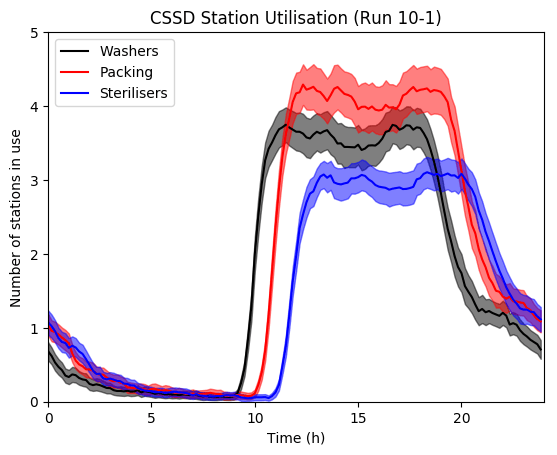
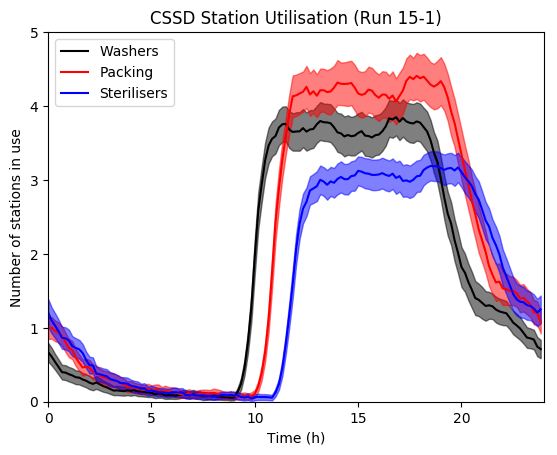
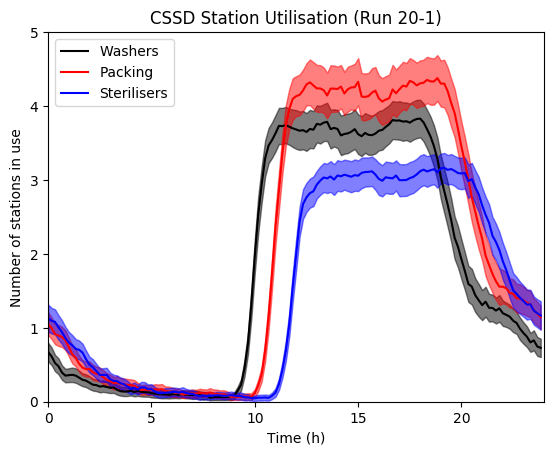
The utilisation of the CSSD may also be of interest to hospitals. Amongst other outputs, this can also be monitored using the simulation model.
Here, the average number of washers, packing tables, and sterilisers in use over the duration of a day is plotted. As the number of instrument sets are increased, there is an increase in the utilisation of the CSSD Stations.
A demand profile becomes prominent after a certain inventory level. During the peak hours of usage, between about 10am-8pm, the washers and sterilisers typically reach their capacity, causing bottlenecks in the CSSD.
Conclusions
- A simulation model has been developed to reflect the usage of reusable medical equipment in hospitals.
- The simulation has demonstrated the proof of concept that the inventory level required to achieve a desired service level can be determined.
- Achieving a high service level comes at the expense of high cost. Hospitals will need to consider both cost and service level when determining the best number of equipment sets to have available.
In the future, this simulation framework can be used to evaluate the effect of other methods that could be used to improve the management of RME. For example, optimising the surgical schedule, or changing the CSSD processing policy could be explored.
Project partner: Sherwyn D’Souza
Supervised by: Dr. Michael O’Sullivan

As part of ENGSCI700 Research Project
Department of Engineering Science
The University of Auckland